How Dermacuro’s Pain Blocker VNDD works
HOW DOES THE BRAIN SENSE DIFFERENT STIMULI?
There are different nerve types that convey sensations to the brain:
Painful sensations such as a needle prick, stepping on a sharp object or a cut in the skin are carried along small-diameter nerves (nociceptors).
Non-pain type sensory information such as cold, heat, texture, vibration are carried along large diameter nerves (non-nociceptors).
The different nerves and the forwarded signals have their individual pathways to the brain, so the brain can register if the signal is detecting potential harm or not.

HOW DOES THE BRAIN PERCEIVE PAINFUL STIMULI?
Nociception is a term used to describe the detection of painful stimuli. Nociceptors are specific receptors within the skin, muscle, skeletal structures, and viscera that detect potentially damaging stimuli. The nociceptive inputs are designed to alert the brain of potential dangers that could cause harm – eg: skin penetration resulting from cutting or pricking, extreme heat, cold, mechanical, or chemical signals.
HOW DOES THE BRAIN PERCEIVE NON-PAINFUL STIMULI, EG: VIBRATION?
The sensory conduction pathway functions through afferent neurons, also known as sensory neurons. These neurons carry signals received by mechanoreceptors on the skin's surface through to the brain, allowing for cognitive (conscious) recognition.
HOW DOES THE VNDD WORK TO REDUCE PAIN?
Perception of pain is not simply due to the activation of nociceptors but is the outcome of the summation of both nociceptive and non-nociceptive inputs. If nociceptive (painful) signals outweigh non-nociceptive (non-painful) signals, a pain signal is propagated to the brain. However if non-nociceptive (non-painful) signals outweigh nociceptive (painful) signals, the pain signal to the brain is reduced.
Pain sensation can usually be reduced by activating a non-painful sensation (vibration) close to where the pain is being felt.

Patients are more likely to return for repeat procedures when they are less anxious about the pain associated with the procedure.
OUR DEVICE UTILISES THE NEURON DISTRACTION METHOD DESCRIBED IN THE GATE CONTROL THEORY OF PAIN
Although each forwarded signal has its individual pathway to the brain via its respective nerve type, the painful sensation nerve pathway can be disrupted by being occupied with receiving signals from the non-pain nerve pathway.
This ‘disruption’ or ‘distraction’ is possible because of a neuron connection between the small (pain) and large (non-pain) neurons within the spine. This connection is known as the ‘inhibitory interneuron’.
According to the Gate Control Theory of Pain, inhibitory interneurons regulate the transmission of ascending nociceptive (painful) information at the level of the second-order neuron, allowing for modulation of the pain signal forwarded to the brain.
UNMODULATED PAIN

MODULATED PAIN
THE GATE CONTROL THEORY OF PAIN IN MORE DETAIL
The basic principle of the Gate Control Theory is that ascending nociceptive signals can be suppressed by the activity of inhibitory interneurons, which function as ‘gates’ to modulate the transmission of the pain sensation by the second-order neurons.
When pain is not modulated, the activation of the C fibre causes excitation of the second-order neuron and, because the 'gate is open’, the nociceptive information of pain sensation is forwarded up the spinal column to the brain where the pain signal is registered and consciously 'felt'.
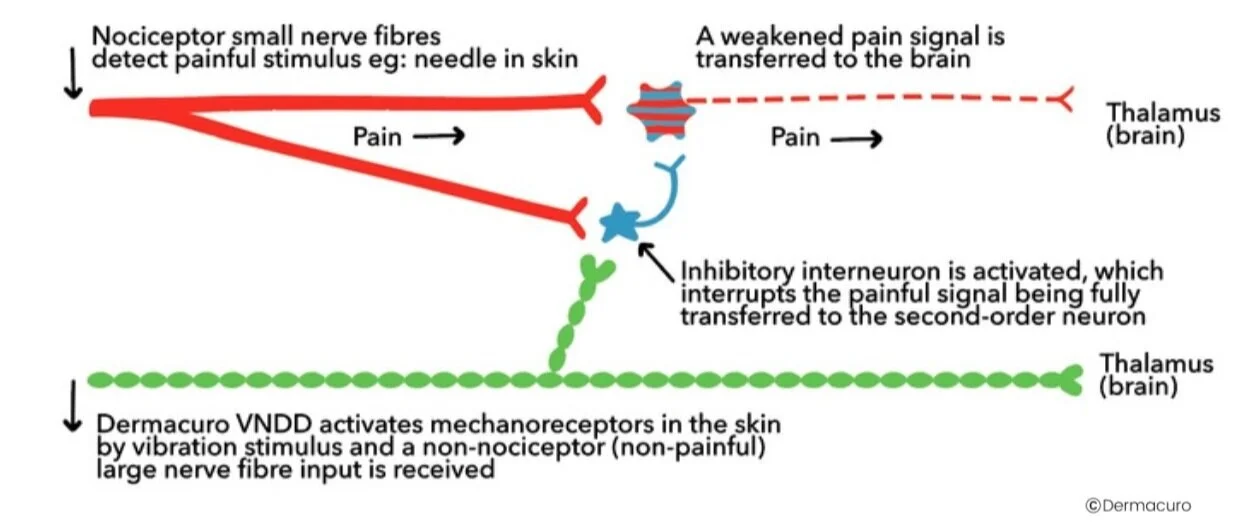
When pain is modulated by simultaneous vibration close to the pain sensation site, the local mechanoreceptors are activated. This activation of the non-nociceptor (non-painful) Aβ fibre, in turn, activates the inhibitory neuron, interrupting the nociceptor (painful) signal from passing to the second-order neuron and effectively decreasing the flow of nociceptive (painful) signals. The action of the inhibitory neuron ‘closes the gate’ and disrupts the onward motion of the painful signal which significantly reduces the volume of nociceptive signals travelling through the spinal cord and therefore the registration of pain by the brain.
There are many simple examples of the use of this theory in pain modulation. Consider the action of automatically rubbing an elbow that has been bumped: we know instinctively that rubbing the skin beside an area of pain will ease the pain we are experiencing. Rubbing the skin activates large-diameter neurons associated with mechanoreceptors, subsequently increasing inhibitory interneuron activity which works to ‘close the gate and decrease the volume of pain signals received by the brain.

The Dermacuro Pain Blocker VNDD can help to reduce paediatric patient anxiety associated with immunisations